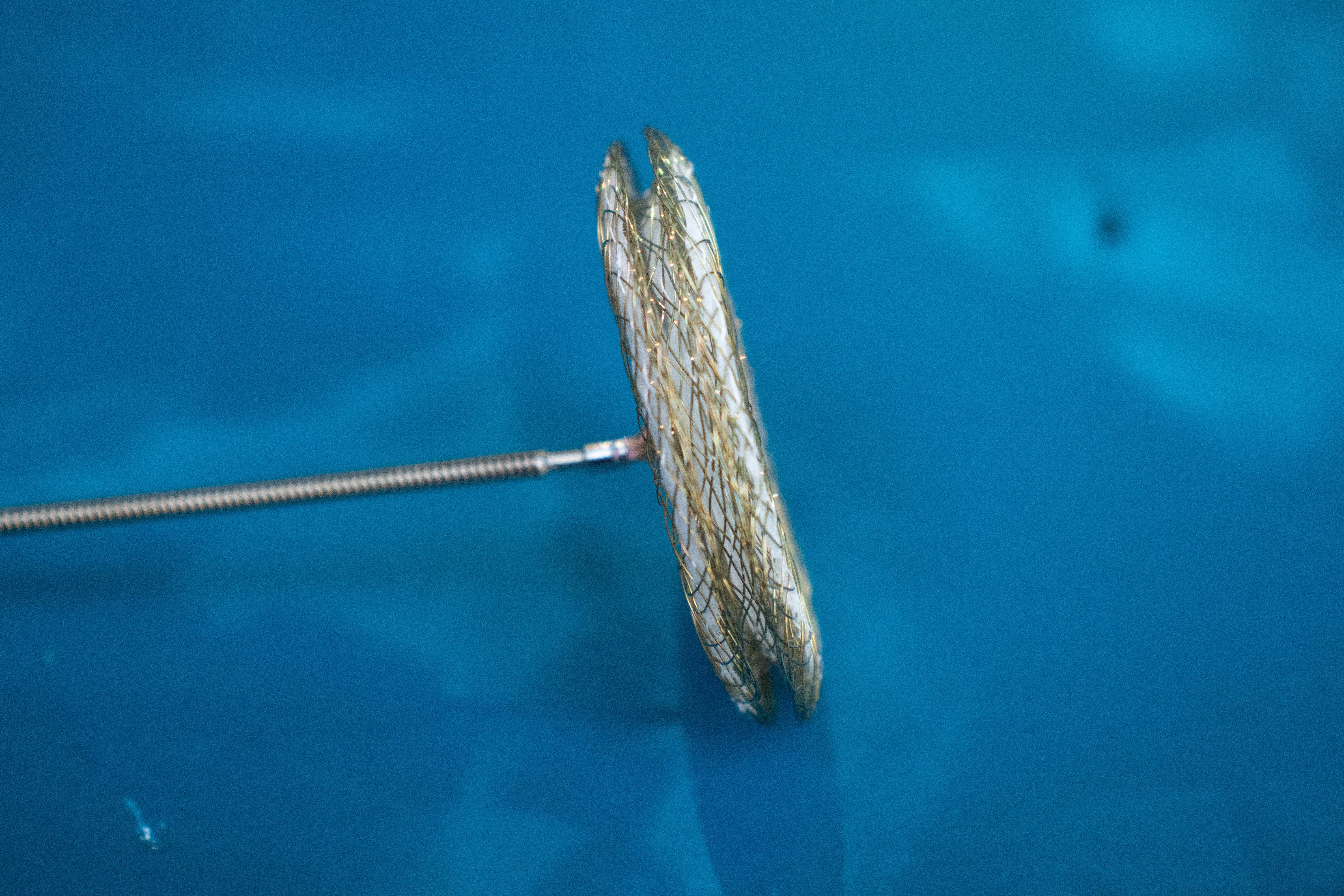
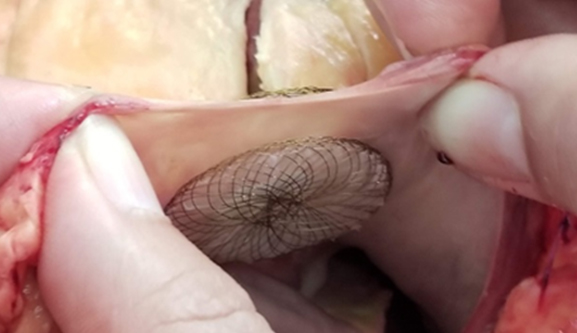
VSO Devices are the standard of care for minimally invasive
Atrial Septal Defect (ASD) closure. These double-disc occluders are comprised of nitinol mesh and ePTFE material. They are designed to securely oppose the septal wall on each side of the defect and create a platform for tissue in-growth after implantation.
Different Occluders for Different sizes of ASD
Variations DOES NOT Matter
Atrial septal defects come in a variety of shapes and sizes. They can often be multiple, or fenestrated, mal-aligned, or spiral ASDs with variation in special orientation. HeartX offers a unique model of Versatile percutaneous, transcatheter occluders that can close any morphologic variation of all these different types of atrial septal defects.
Atrial Septal Defect (ASD) is a common birth defect involving the heartin which there is a hole in the partition between the two collecting chambers of the heart, known as Atria. Standard of care for ASD closure is through transcatheter approach. There is a prevalence of 1.5 to 2 million patients with ASD and yearly incidence is 37,500 in India.
About 900-1000 ASD Devices are implanted in India. Currently available devices have major defi- ciencies which led us to develop the VSO device
Advantages of VSO
Most advanced and versatile device for ASD closure
today.
It utilizes experience of currently available devices and its potential for improvement. The device is made of nitinol with shape memory properties which has been used in similar devices across the world, with established safety profile in human heart.
Improved design, safety profile and ease of use.
Only 8 devices needed to cover all sizes and morphology of ASD varia- tions compared to current versions needing 18 devices.
Less Risk of Complications:
Versatile to adjust to the variations in the nature of the defects. Minimal risk of embolization or erosion.
No need for balloon sizing.
One size fits many! Ease of deployment with minimal or no flouroscopy and even can be performed under trans-thoracic echocardiography.
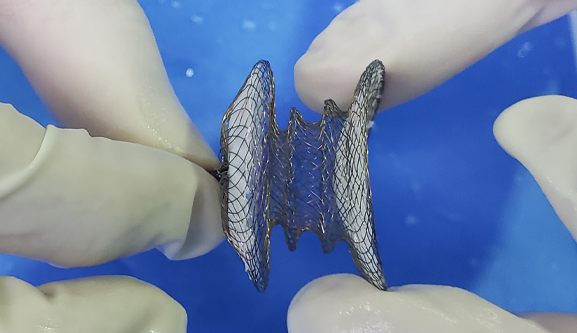
Uniqueness of VSO
- Device in device = stability: Many devices compacted. 2-3 sizes in one device
- Central anchoring reduces retention force away from the LA/RA discs
- Variable conjoined rings of graded diameters give versatility
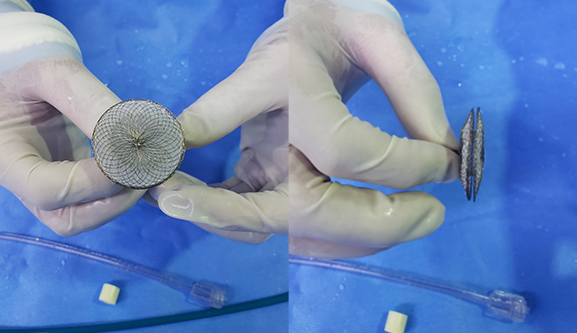
- Smaller LA disc (D1) provides less metal surface
- Highly flexible LA/RA discs
- Longer device profile prior to deloyment prevents disc protrusion and “buttonhole”
- Avoids malposition and better maneuverability.
- Smaller disc size provides better device profile which reduces sheath size.
- Softer device profile means less risk of erosion and flexible anchoring.
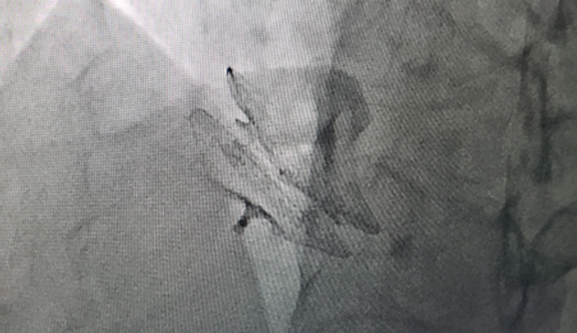
- Post-deployment flouroscopy image of VSO
Ordering Information
|
Sl no
|
Model/Reorder Number |
Waist Diameter (mm) |
Waist Width (mm) |
RA/LA Disc Diameter (mm) |
| 1 |
9-VSO-6-10 |
6,8,10 |
3 |
22 |
| 2 |
10-VSO-12-14 |
12,14 |
3 |
26 |
| 3 |
11-VSO-16-18 |
16,18 |
3 |
30 |
| 4 |
12-VSO-20-22 |
20,22 |
3 |
34 |
| 5 |
12-VSO-24-26 |
24,26 |
3 |
38 |
| 6 |
12-VSO-028-30 |
28,30 |
3 |
42 |
| 7 |
14-VSO-032-36 |
32,34,36 |
3 |
48 |
| 8 |
14-VSO-38-42 |
38,40,42 |
3 |
54 |
Indications for Use
The Versatile Septal Occluder Device is a percutaneous, transcatheter, atrial septal defect closure device intended for the occlusion of atrial septal defects (ASD) in secundum position or patients who have undergone a fenestrated Fontan procedure and who now require closure of the fenestration. Patients indicated for ASD closure have echocardiographic evidence of ostium secundum atrial septal defect and clinical evidence of right ventricular volume overload (such as, Qp/Qs of >1.5 or RV enlargement).
Contraindications
The VASO Device is contraindicated for the following:
- Any patient known to have extensive congenital cardiac anomaly which can only be adequately repaired by way of cardiac surgery.
- Any patient known to have sepsis within 1 month prior to implantation, or any systemic infection that cannot be successfully treated prior to device placement.
- Any patient known to have a bleeding disorder, untreated ulcer, or any other contraindications to aspirin therapy, unless another antiplatelet agent can be administered for 6 months.
- Any patient known to have a demonstrated intracardiac thrombi on echocardiography (especially left atrial or left atrial appendage thrombi).
- Any patient whose size does not allow the passage of the delivery system or the procedure would cause hemodynamic instability.
- Any patient where the margins of the defect are less than 5 mm to the coronary sinus, inferior vena cava rim, AV valves, or right upper lobe pulmonary vein.
Warnings
- Physicians must be prepared to deal with urgent situations, such as device embolization, which require removal of the device. This includes the availability of an on-site surgeon.
- Embolized devices must be removed as they may disrupt critical cardiac functions. Embolized devices should not be withdrawn through intracardiac structures unless they have been adequately collapsed within the sheath.
- Use on or before the expiration date noted on the product packaging.
- This device is sterilized using ethylene oxide and is for single use only. Do not reuse or resterilize. Attempts to resterilize the device may result in device malfunction, inadequate sterilization, or patient harm.
- Do not use the device if the packaging sterile barrier is open or damaged.
- Do not release the VASO Device from the delivery cable if the device does not conform to its original configuration, or if the device position is unstable or if the device interferes with any adjacent cardiac structure (such as Superior Vena Cava (SVC), Pulmonary Vein (PV), Mitral Valve (MV), Coronary Sinus (CS), aorta (AO)). Recapture the device and redeploy. If still unsatisfactory, recapture the device and either replace with a new device or refer the patient for alternative treatment.
- The use of echocardiographic imaging (TTE, TEE, or ICE) is required.
- Patients with a retro-aortic rim of less than 5 mm in any echocardiographic plane, or patients in whom the device physically impinges on (i.e. indents or distorts) the aortic root, may be at the potential risk of erosion.
- Select only devices within the recommended range for the device.
Precautions
- Use standard interventional cardiac catheterization techniques to place this device.
- Placement of the VASO Device may impact future cardiac interventions, for example transeptal puncture and mitral valve repair.
- This device contains nickel-titanium alloy, which is generally considered safe. Patients who are allergic to nickel may have an allergic reaction to this device, especially those with a history of metal allergies. Certain allergic reactions can be serious; patients should be instructed to seek medical assistance immediately if they suspect they are experiencing an allergic reaction. Symptoms may include difficulty in breathing or swelling of the face or throat. While data is currently limited, it is possible that some patients may develop an allergy to nickel if this device is implanted.
Handling
Store in a dry place.
Procedural
- This device should only be used by physicians who have been trained in transcatheter techniques and who should determine which patients are suitable candidates for procedures using this device.
- The physician should exercise clinical judgment in situations that involve the use of anticoagulants or antiplatelet drugs before, during, and/or after the use of this device.
- Aspirin (for example, 81 mg) or an alternative antiplatelet/anticoagulant is recommended for 3 months after the device deployment. Antibiotic prophylaxis is recommended to cover the procedure.
- Maintain a recommended minimum active clotting time (ACT) of 200 seconds prior to device insertion and throughout the procedure.
- If TEE is used, the patient's esophageal anatomy must be adequate for placement and manipulation of the TEE probe.
Post-implant
- Patients should take appropriate endocarditis prophylaxis for 6 months following device implantation. The decision to continue endocarditis prophylaxis beyond 6 months is at the discretion of the physician.
- Patients should be treated with antiplatelet/anticoagulation therapy (such as aspirin) for 3 months post-implant. The decision to continue antiplatelet/anticoagulation therapy beyond 3 months is at the discretion of the physician.
- Clinical follow-up with a cardiologist and echocardiograms are recommended at implant, 1 day post-implant, and again at 6 week, 6 months, and 12 months post-implant. Immediate follow-up with a cardiologist with the onset of any new symptoms suggestive of erosion or impending erosion, and routine clinical follow-up annually thereafter is also recommended.
Use in Specific Populations
- Pregnancy – It is safe to do the implantation of VASO device provided no or minimal radiation exposure to the fetus and the mother.
- Nursing mothers - There has been no quantitative assessment of the presence of leachables from the device/procedure in breast milk, and the risk to nursing mothers is unknown.
MR Conditional to 3.0 Tesla
Caution should be used if an MRI is performed with a magnetic field of >3.0 tesla. Through non-clinical testing, VASO device has been known to be MR Conditional at field strengths of 3.0 tesla or less. The VASO device should not migrate in this MR environment. Non-clinical testing has not been performed to rule out the possibility of migration at field strengths higher than 3.0 tesla.
MR image quality may be compromised if the area of interest is in the exact same area or relatively close to the position of the device.
Potential Adverse Events
Potential adverse events may occur during or after a procedure placing this device may include, but are not limited to:
- Air embolus
- Allergic dye reaction
- Anesthesia reactions
- Apnea
- Arrhythmia
- Cardiac tamponade
- Death
- Embolization
- Fever
- Hypertension/hypotension
- Infection including endocarditis
- Need for surgery
- Pericardial effusion
- Perforation of vessel or myocardium
- Pseudoaneurysm including blood loss requiring transfusion
- Tissue erosion
- Thrombus formation on discs
- Stroke
- Valvular regurgitation